This infographic shows the relationship between ACEs and toxic stress. This relationship has implications for our children with special needs.

5 Reasons to Blog During PTSD Awareness Month
5 Reasons to Blog During PTSD Awareness Month
June is PTSD Awareness Month, and though I sometimes feel there’s nothing more for me to write on post traumatic stress disorder, here I am blogging about it again. Specifically about PTSD in children, also known as childhood developmental trauma. Here are 5 reasons this topic is worth writing about year after year.
Reason #1: Too Many Children Suffer from PTSD
Exact numbers are hard to pin down, but as this report from the National Center on PTSD, more children live with PTSD than we’d like to think, definitely in the tens and hundreds of thousands. But even if only one child was living with untreated PTSD, that’s one child too many.
Reason #2: PTSD in Children is Highly Preventable
All children experience trauma at some point in life, but not all children develop post traumatic stress disorder. PTSD happens when a child experiences a trauma and the emotions and physical sensations accompanying the traumatic event become trapped in. Research shows that after a traumatic event, PTSD usually doesn’t develop in children who, with the help of a calm and supportive adult, are able to process the trauma, leave it in the past, and move on.
Reason #3: PTSD in Children Is Highly Treatable
Even when children whose unprocessed trauma becomes PTSD, all is not lost. Children as young as three can receive effective trauma treatment. The best methods are those that are not talk-based, and the best therapists have at least some training that is trauma-focused. For a thorough look at treatment methods, I recommend The Body Keeps the Score. In it Bessel van der Kolk describes and reviews the research related to dozens of trauma therapies.
Reason #4: Without Treatment Childhood PTSD Leads to Complications
The earlier a child is diagnosed with PTSD and receives treatment, the better. The longer treatment is delayed, the more likely the condition is to become a more complex mental illness called dissociative disorder. Also, a study called The Adverse Childhood Experiences Study (ACES) revealed that children who experience traumatic events that are left untreated are likely to become adults who struggle to maintain healthy relationships, develop serious health concerns, and have shorter lifespans.
Reason #5: My Son Lived with Untreated PTSD for 26 Years
Our son developed PTSD after 4 years of invasive, painful surgeries and medical procedures that began on the day of his birth in 1982. His diagnosis came in 2008 when he was 26, and after a week of intensive, outpatient trauma therapy, he looked at me and said, “For the first time in my life, I’m not looking over my shoulder waiting for someone to take me into surgery.” My heart leaped for joy to know that he had found relief from the terrifying, wordless memories that had plagued him for decades. Simultaneously, a resolve grew within me to tell other families about PTSD so their children wouldn’t have to wait 26 years to find relief in treatment.
Ten years later the resolve is as strong as ever, and I invite you to join me in raising awareness about PTSD in children until traumatized children receive the help and effective treatment they need.
Do you like what you see at DifferentDream.com? You can receive more great content by subscribing to the quarterly Different Dream newsletter and signing up for the daily RSS feed delivered to your email inbox. You can sign up for the first in the pop up box and the second at the bottom of this page.
By
Jolene Philo is a published author, speaker, wife, and mother of a son with special needs.
Author Jolene Philo

Subscribe for Updates from Jolene
Related Posts
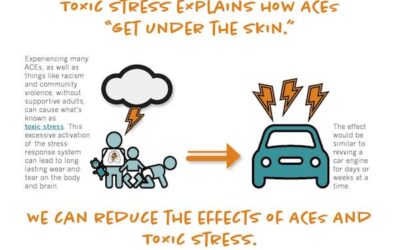
The ACEs and Toxic Stress: Implications for Children with Special Needs?
read more

Preventing PTSD: 11 Things To Do If Your Child Has Been Through Trauma
Preventing PTSD in children who have experienced trauma is possible. Lydia Jenkins, D.O. Pediatrics offers 11 strategies for parents to use.

More Than Words: The Freedom to Thrive After Trauma
The author of More Than Words: The Freedom to Thrive After Trauma explains why she wrote the book and how she made a heavy topic easy for readers to digest.